
Medical marijuana is the whole, unprocessed marijuana plant or the chemicals contained within it to alleviate the symptoms of certain conditions or diseases. The plant is comprised of over 100 chemicals or cannabinoids. Each has different effects on the body. The first main chemical is tetrahydrocannabinol or THC. This is the psychoactive compound in marijuana, i.e., the element that produces the high. The second is cannabidiol or CBD. This substance does not produce any psychoactive effects. Medical marijuana has a higher CBD content, so users do not feel the euphoria associated with recreational marijuana. Recreational marijuana usually has more THC content than the medicinal variety, as this is what provides users with a “high.”
How is medical marijuana administered and dosed? Whole-plant cannabis is smoked or vaped, extracts are oromucosal sprays, and synthetics are taken orally in pill form.
The therapeutic range of cannabinoids is small; often small doses are enough for clinically significant pain reduction. A 2014 study compared two doses of cannabis (medium dose, 3.5 percent THC, to low dose, 1.3 percent THC) to see if the pain relief from the low dose was enough to recommend using lower doses to avoid side effects. It was.
To achieve the full effect on pain reduction, patients may need to repeat doses of medical marijuana more often than doses of other medications. In a small study of patients with allodynia and hyperalgesia, abnormally increased sensitivity to pain, authors analyzed pain reports three hours and eight hours after taking medication. Those in the study drug group reported less pain three hours after taking their drug than those who had the placebo drug. Eight hours after intake of the drug, the reported pain differences between groups were less marked.
What else is known about side effects or adverse events? Both non-serious and severe side effects were higher in patients using medical marijuana than patients in placebo groups. (Note that placebos are usually medications conventionally used for neuropathic pain, not sugar pills.) Patients in the marijuana groups reported dizziness most often. Other common side effects include dry mouth, nausea, disorientation, euphoria, confusion, sedation, and increased heart rate, which may increase the chance of heart attack in people who are already at risk. Severe side effects were dyspnea, pneumonia, pleural effusion, lower respiratory tract infection, and pulmonary embolism; vomiting, diarrhea, gastroenteritis, abdominal pain, constipation, duodenal ulcer; and convulsions. Regular smoking of marijuana is associated with breathing problems such as a cough and increased risk of lung infections. Gastrointestinal adverse effects occurred more often when the medicines were taken orally rather than inhaled. Many authors noted that the medications used to treat chronic pain are have some of the same side effects. Medical marijuana and placebos did not differ in terms of safety during the study period. Cannabinoids are well tolerated by patients and tolerance to their beneficial effects does not develop.
Continuous long-term use of cannabis is associated with harmful effects on bone mineral density, leading to an increased risk of bone fractures. This concerning for people who may need neurosurgery. Neurosurgeons must take extra care with instruments in these patients.
Summary of Findings:
Medical marijuana shows promise for relief of chronic, neuropathic pain. Though, the amount of relief varies from study-to-study. Overall, studies show that it offers low to moderate pain relief. Some studies show considerable pain relief, while others show none. Medical marijuana relieved pain no matter where in the body the pain occurred. However, there has not been a study that focused specifically on orofacial pain.
Scientists believe that medical marijuana can address allodynia, abnormal pain from normal sensations such as light touch, slight temperature changes, or gentle brushing of the skin. Endocannabinoids are neurotransmitters which send signals through the brain. These signals are important for many functions in the human body including those involving mood, pain, and inflammation. Endocannabinoids could be early players in bringing on allodynia. Using medicines to regulate the endocannabinoid system could be a breakthrough in treating neuropathic pain that is untreatable with commercially available
Studies suggest that patients try other treatments with higher levels of evidence before turning to medical marijuana. A pharmaceutical study classified cannabinoids as 4th level treatment behind other medications such as anti-epileptic drugs, tricyclic antidepressants, topical lidocaine, selective serotonin-norepinephrine reuptake inhibitors, and even opioid analgesics.
How cannabinoids should be taken, their optimal doses, and which type of cannabinoids would be effective with fewest side effects are still questions to be answered. The evidence for using cannabinoids specifically for orofacial pain is absent. We need
“Are Cannabinoids Effective for Orofacial Pain States?” 2015. Barry Sessle is the editor-in-chief of the Journal of Orofacial Pain and Headache. He wrote an editorial review of the Boychuk article. He noted that the main focus of the research on cannabinoids for
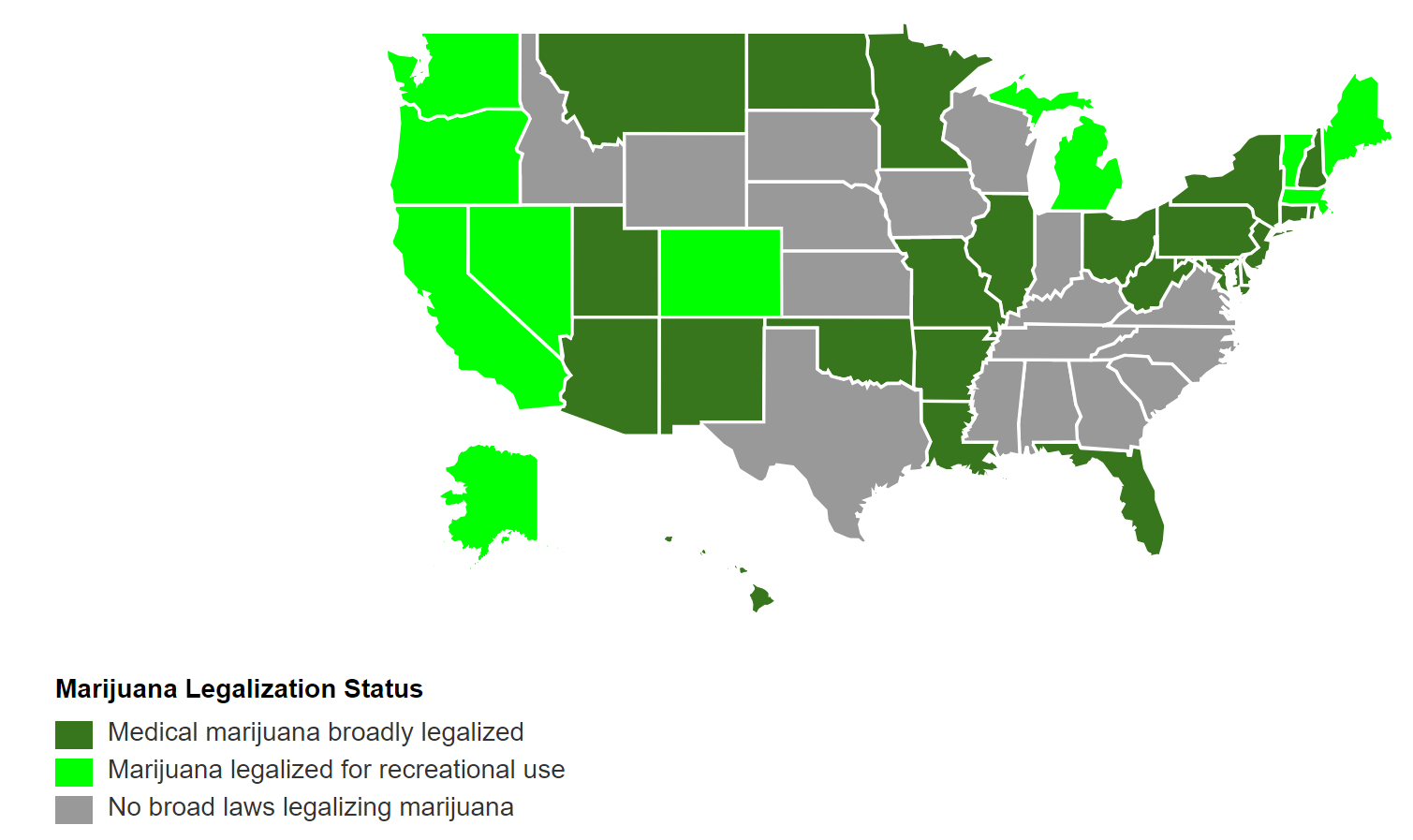
The map shows current state laws and recently-approved ballot measures legalizing marijuana for medical or recreational purposes. Final rules for recently-passed medical marijuana laws are pending in some states. Information is current as of Nov. 7, 2018.
http://www.governing.com/gov-data/state-marijuana-laws-map-medical-recreational.html
Credit for Blog goes to Fall-Winter 2018 Quarterly:
Journal of the Facial Pain Association

- Women and Estrogen and Prevalence in Temporomandibular Disorders - October 11, 2024
- DRY MOUTH (Xerostomia) - August 10, 2024
- 4-7-8 Breathing For you - May 22, 2024